如何预测Danis-Weber B型踝关节骨折下胫腓联合损伤?
时间:2021-10-11 18:03:14 热度:37.1℃ 作者:网络
Lauge-Hansen分型与Danis-Webe分型为最常见的踝关节骨折分型,在对下胫腓韧带损伤的指导意义上,旋后外旋II°骨折通常认为合并下胫腓前韧带的损伤,下胫腓联合趋于稳定,可能无需下胫腓联合螺钉固定。而Danis-Weber B型骨折定义为骨折位于下胫腓联合水平,可能合并下胫腓联合损伤。
由此可发现,对Danis-Weber B型骨折,如何评估下胫腓有无损伤,以及术前评估是否需手术固定下胫腓联合,仍无有效参考。
对此,国外学者研究了Danis-Weber B型近端骨折线的位置,以求对比不同类型B型骨折下胫腓联合损伤比例是否存在差异,并指导手术干预。
Objective(目的)
确认术前X线检查能否预测下胫腓联合损伤几率。[Objective: To establish if preoperative radiographs could predict the rate of syndesmotic injury.]
Patients/participants(病例)
回顾了548例 OTA/AO 44-B2.1型患者,287例患者纳入研究。 [Patients/participants: There were 548 OTA/AO 44-B2.1 fractures that were reviewed, and 287 patients were included in the study.]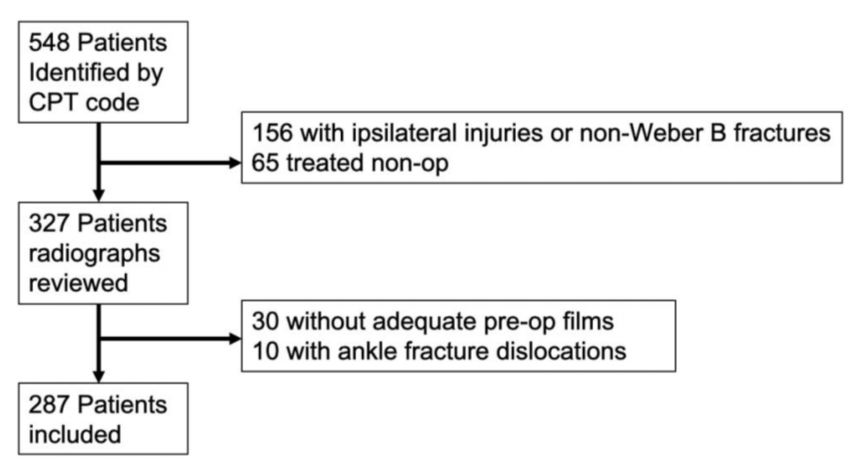
图1 病例纳入流程。
Main outcome measures(主要结局指标)
踝关节影像片用于明确近端骨折块的远端范围。下胫腓联合损伤定义为术中压力试验证实并需要下胫腓固定。
[Main outcome measures: Ankle radiographs were used to determine the zone of distal extent of the proximal fracture fragment. Syndesmotic injury was defined as positive intraoperative stress examination that required syndesmotic fixation.]
图2 Danis-Weber B型骨折,根据近端骨折块最远端位置分区。1区定义为骨折块最远端位于胫骨远端关节面平面以下;2区为位于胫骨远端骺线闭合瘢痕与远端关节面之间;3区为骺线闭合瘢痕以上。

图3 分区示意图。
Results(结果)
共有191例1区(止于胫骨远端关节平面下方)损伤,57处2区(止于胫骨远端骨骺线闭合瘢痕和胫骨远端关节面之间)损伤,39处3区(止于胫骨远端骨骺线闭合瘢痕以上)损伤。其中,17% (33名患者)的1区、42% (24名患者)的2区和74% (29名患者)的3区骨折合并下胫腓韧带损伤。
2区与1区相比,韧带联合损伤的相对风险为2.4 (P,0.001),3区与1区相比为4.3 (P,0.001),3区与2区相比为1.8 (P = 0.002)。观察者间和观察者内的可靠性非常好(k = 0.86,0.94)。
[Results: There were 191 zone 1 (ending below the plafond) injuries, 57 zone 2 (ending between the physeal scar and the plafond) injuries, and 39 zone 3 (ending above the physeal scar) injuries. Of these, 17% (33 patients) of zone 1, 42% (24) of zone 2, and 74% (29) of zone 3 fractures had syndesmotic injuries. The relative risk of syndesmotic injury of zone 1 compared with zone 2 was 2.4 (P , 0.001), zone 1 to zone 3 was 4.3 (P , 0.001), and zone 2 to zone 3 was 1.8 (P = 0.002). The interobserver and intraobserver reliability was excellent (k = 0.86, 0.94).]

Conclusion(结论)
OTA/AO 44-B2.1骨折具有不同的下胫腓联合损伤率。Weber B型骨折发生在胫骨远端关节平面和骺线闭合疤痕之间(2区),与发生在关节面下方(1区)的骨折相比,发生韧带损伤的可能性高2.4倍。这种可能性在骺线闭合疤痕上方(3区)的损伤中更大。
OTA/AO 44-B2.1骨折的简单分类预示着韧带损伤,可能有助于术前咨询和手术计划制定。
[Conclusion: OTA/AO 44-B2.1 fractures have a varying rate of syndesmotic injury. Weber B fractures that end between the level of the plafond and the physeal scar (zone 2) are 2.4 times more likely to have a syndesmotic injury compared with those that end below the plafond (zone 1). This is magnified in those injuries ending above the scar (zone 3). This simple classification of OTA/AO 44-B2.1 fractures is predictive of syndesmotic injury and may aid in preoperative counseling and planning.]

